

The gradual generalization of Mandatory Health Insurance (AMO) has ushered Morocco’s healthcare system into a new phase. By rapidly expanding the covered population, the reform has led to a significant increase in expenditures borne by managing bodies, foremost among them the National Social Security Fund (CNSS).
In this context, drugs have emerged as one of the main spending items of health insurance. In 2024, they account for more than one-third of reimbursements made by the CNSS, confirming the structural weight of pharmaceuticals in the scheme’s financial balance.
This dynamic highlights a lever long viewed as technical but now central: the model for setting the public selling price (PSP) of drugs. Designed in a context that predates the generalization of AMO, this model is now facing new pressures, as reimbursed volumes increase and spending becomes concentrated on a limited number of treatments.
A system under strain
Before addressing the reform, a look back at the existing mechanism. Drug pricing in Morocco is based on a regulatory framework structured around two decrees that remain in force. These texts form the legal backbone of the national policy on drug pricing and reimbursement.
Decree No. 2-13-852 governs the procedures for setting and revising drug prices. In particular, it defines the determination of the manufacturer’s price excluding tax (PFHT), which serves as the basis for calculating the public selling price (PPV). Decree No. 2-05-733, for its part, sets out the rules for drug reimbursement by the bodies managing AMO, specifying the applicable bases and rates, notably depending on whether or not the treatments fall under long-term conditions. Together, these two texts structure the entire pricing and reimbursement chain.
Within this framework, the PPV is built on three components: the manufacturer’s price excluding tax (PFHT), to which are added the wholesaler’s margin and the pharmacy’s margin, both calculated on the basis of the PFHT. This mechanism directly links the level of the final price to the manufacturer’s price, which plays a central role in the overall structure of prices applied on the national market.
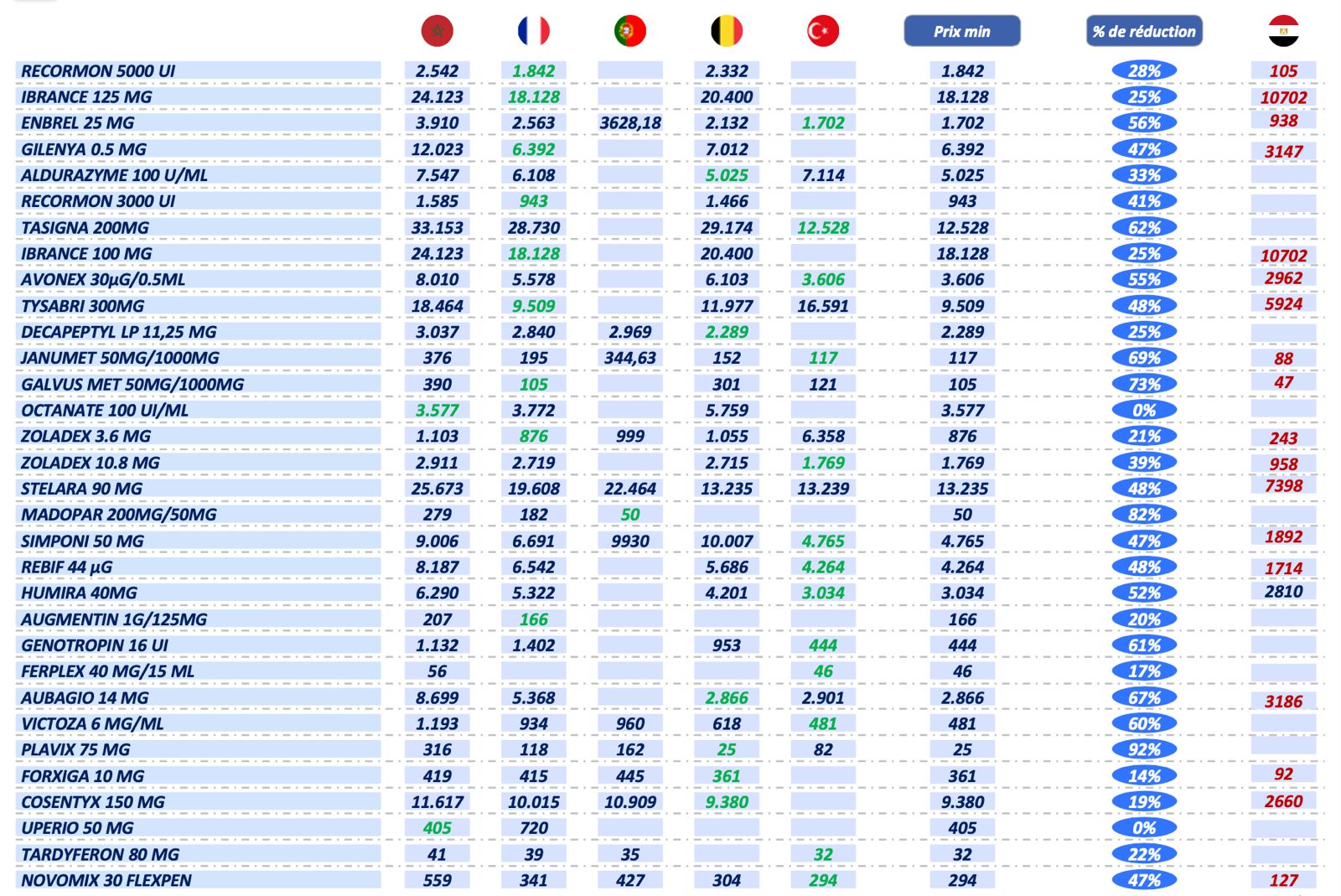
For originator drugs, the PFHT is initially set by retaining the lowest price observed in a group of reference countries, namely France, Belgium, Portugal, Spain, Turkey, and Saudi Arabia, as well as in the country of origin of the drug when this is different. During price revision operations, the mechanism changes: the PFHT retained then corresponds to the average of the prices observed in these reference countries.
This benchmarking mechanism had already been examined by TelQuel in a feature published in 2020, which documented the price gaps observed between Morocco and France for identical drugs, and their impact on reimbursement bodies. In that feature, an internal CNOPS study obtained by TelQuel highlighted significant differentials across 33 references, with gaps exceeding 250% in some cases.
The same feature recalled that, since the 2014 reform, the price of new originator drugs has been based on this international comparison, with the price set on the basis of the lowest level observed in the basket of countries. But TelQuel emphasized at the time that, despite this principle, prices remained high for many references, notably due to the profile of the reference countries, characterized by income levels bearing no comparison to national purchasing power.
Added to this framework, for imported drugs, is a 10% markup on the PFHT, intended to cover the importer’s margin, handling costs, and customs duties. A mechanism that contributes to driving up the final price regardless of the drug’s therapeutic use, and that mechanically weighs on the amounts reimbursed by AMO managing bodies.
Limited safeguards
The pricing of generic drugs is based on the application of minimum reduction rates relative to the PFHT of the reference originator, which vary depending on the price bracket. These floor thresholds nevertheless leave laboratories with significant room for maneuver in determining final prices, according to documents reviewed by TelQuel.
In practice, this framework does not impose automatic convergence toward the least expensive alternatives. Several price levels can therefore coexist for the same molecule, with no systematic mechanism pushing prices downward, according to the same sources.
On the reimbursement side, the reference price retained generally corresponds to the PPV, including when generics exist. Reimbursement is then calculated on the basis of the most expensive generic, which limits the moderating effect expected from generic competition on health insurance spending. Added to this are the absence of targeted and regular revisions, the slowness of reimbursement admission procedures, and the lack of delisting mechanisms, which make drug spending more rigid.
A polarized system
This pricing framework produces structural effects on pharmaceutical spending. As revealed by TelQuel in a previous article, drug reimbursements by the CNSS reached 3.8 billion dirhams in 2024, in a context of the gradual generalization of AMO.
These amounts are highly concentrated. A significant share of reimbursements concerns a limited number of drugs, mainly costly treatments linked to severe and chronic conditions. This concentration is also observed at the level of therapeutic classes, dominated by a few high value-added segments.
It is also reflected at the level of beneficiary laboratories, mostly international or operating under license, which capture the bulk of reimbursed amounts. The generalization of AMO, implemented from late 2022 onward, acted as an accelerator, with drug reimbursements increasing by around 30% since that date. This configuration explains why the authorities are now favoring a targeted reform, rather than a uniform revision of prices across the entire market.
Addressing blind spots
The diagnosis is now widely shared within the healthcare system, including by the Minister of Health and Social Protection, Amine Tehraoui: the current pricing model is now showing its limits in a system undergoing rapid scale-up. Designed in a context where reimbursed volumes remained relatively contained, this framework appears increasingly ill-suited to the rapid generalization of AMO and the continuous expansion of the covered population.
One of the main blind spots of the system lies in the absence of levers allowing for targeted action on the most budget-intensive drugs. The current system is based on general rules for price setting and revision, with no specific mechanism to correct imbalances caused by a limited number of medicines accounting for a disproportionate share of reimbursements. This rigidity weighs directly on the financial balances of health insurance, particularly those of the CNSS.
As the generalization of AMO becomes more firmly established, pharmaceutical spending per capita is set to rise mechanically, increasing the pressure on the fund’s finances
As the generalization of AMO becomes more firmly established, pharmaceutical spending per capita is set to rise mechanically, increasing the pressure on the fund’s finances. Maintaining the current framework, without targeted adjustment, therefore appears increasingly difficult to sustain over the medium term, both from a budgetary standpoint and in terms of the scheme’s sustainability.
It is in this context that a far-reaching revision of the price-setting model has moved onto the agenda of the health authorities. According to documents consulted by TelQuel, they are proposing a new integrated model designed to correct the observed imbalances without calling into question either access to treatments or the stability of the pharmaceutical supply chain.
At the heart of this reform is a targeted intervention on the most budget-intensive drugs, identified as the main contributors to runaway reimbursements. Unlike the general revisions carried out in the past, the new model favors a selective approach, focused on reimbursed drugs representing the highest amounts for health insurance.
Proof in the numbers
According to simulations carried out by the CNSS and consulted by TelQuel, applying this model to the 32 most expensive originator drugs in the private sector would make it possible to generate substantial savings. These 32 references alone account for around 1.03 billion dirhams in reimbursements. The combined application of the two levers of the new model, namely the reduction of PPVs and the introduction of a negotiated discounted price, would bring this amount down to around 367 million dirhams, representing potential savings of 661 million dirhams, equivalent to a 64% reduction in reimbursements over this limited scope.
In detail, nearly two-thirds of these savings, around 660 million dirhams, would be linked to downward revisions of PPVs, based on alignment with the lowest prices observed in the reference countries. The remaining third would come from the negotiation of a discounted price, distinct from the PPV, applied from the first reimbursed unit and subsequently rebated to the CNSS by the laboratories concerned.
The simulations also highlight a direct impact on insured patients’ out-of-pocket costs. The reduction of PPVs alone would generate a potential savings of around 80 million dirhams for patients, reflecting a tangible reduction in “out of pocket” (personal expenses) without any modification of wholesalers’ and pharmacies’ margins, which are explicitly maintained under the new framework.
The close-up carried out on the prices adopted for these 32 drugs reveals very significant price gaps between Morocco and the reference countries, with potential reductions ranging from 14% to more than 90%, depending on the molecule. For several widely reimbursed treatments, the price used in the simulation corresponds to the minimum price observed internationally, confirming the structural nature of the excess costs generated by the current model.
Beyond the immediate budgetary effect, our sources emphasize that this new model also aims to correct a major weakness of the current system: the absence of any real negotiating capacity on the part of the State for drugs already admitted for reimbursement. By introducing an annually negotiated discounted price, the mechanism restores to public authorities a direct lever of action on the most sensitive expenditures, without calling into question the general principles of price setting.
A reform on stand-by
The implementation of this model would involve several institutional actors. The Ministry of Health and Social Protection would ensure overall steering and the overhaul of the legal framework, notably the decree governing price setting. The Moroccan Agency for Medicines and Health Products (AMMPS) would intervene in the setting and periodic revision of prices, while the High Authority for Health (HAS) would be tasked with assessing the essential nature of medicines, defining therapeutic protocols, and steering applications for listing or delisting. The CNSS, alongside the ministry in charge of the Budget, would play a central role in conducting negotiations with laboratories and in assessing the financial impact of the mechanism.
According to the timeline set out in the documents consulted by TelQuel, the new model is expected to enter into force as early as June 2026, with a first wave of PPV revisions covering the 100 most costly medicines in terms of reimbursements, followed by the launch of negotiations on discounted prices and the gradual revision of other medicines on the market.
However, the implementation of this reform remains contingent on the adoption by the Government Council of the decree governing price setting, as well as on the opinion of the Competition Council, which, according to our colleagues at Médias24, is expected to review the text and issue an advisory opinion after consultation with the various stakeholders.
At a time when medicines are emerging as a central determinant of the sustainability of AMO, the overhaul of the price-setting model thus appears as a structuring project, set to durably reshape the balances of Morocco’s healthcare system. What remains now is to translate this technical architecture into effective decisions, within a constrained timeline, as the financial sustainability of AMO becomes a central public policy issue.
Written in French by Younes Saoury, edited in English by Eric Nielson


